The Real Food Pyramid for Metabolic Health, Eat This
Summary
If you feel like you are “eating healthy” but your weight, blood sugar, or triglycerides are not improving, this video’s message is simple: the old, grain heavy pyramid may be backward for most adults. The approach centers on metabolic health and insulin resistance, using a low carbohydrate food pyramid that prioritizes animal source proteins and whole fat dairy, plus fats and oils, with carbs scaled to activity. It also tackles common worries about saturated fat, LDL cholesterol, and red meat, and offers practical ways to apply the pyramid without turning it into a rigid diet.
🎯 Key Takeaways
- ✓This pyramid is framed for metabolic health, not for elite athletic performance, it targets the majority of adults who are insulin resistant.
- ✓The foundation is high quality protein and minimally processed fats (eggs, fish, red meat, whole fat dairy), with carbohydrates adjusted to activity level.
- ✓The video argues that insulin resistance is a key upstream driver of atherosclerotic plaque development, making blood sugar and insulin dynamics central targets.
- ✓Low carbohydrate patterns are presented as nutritionally complete and potentially sustainable, with “keto flu” framed as largely preventable with hydration and electrolytes.
- ✓Concerns about saturated fat, red meat, and LDL are discussed as more nuanced than commonly portrayed, especially when viewed alongside triglycerides, HDL, blood pressure, and inflammation.
Picture this: you start the week determined to “eat clean.” Breakfast is cereal or oatmeal, lunch is a sandwich, dinner includes pasta or rice, and snacks are granola bars because they look healthier than cookies.
Then you get lab work back and it is still not moving in the direction you want. Maybe your fasting glucose is creeping up, your triglycerides are high, your waistline is stubborn, or you feel hungry again an hour after eating.
The perspective in the video “The REAL Food Pyramid: Eat This Instead” is built for that moment.
Instead of focusing on a one size fits all pyramid, the argument centers on metabolic health, especially insulin resistance, and proposes a different food pyramid for the majority of adults in North America.
Did you know? The video highlights an estimate that 93% of US adults have risk factors for metabolic problems or take medications for obesity, diabetes, or heart disease. That framing comes from a widely cited analysis of US metabolic health published in Metabolic Syndrome and Related Disorders showing only a small minority meet optimal metabolic criteria (PubMed recordTrusted Source).
When “healthy eating” is not working anymore
A major theme is that many people are not failing because they lack willpower.
They are following guidance that may not match their physiology, their activity level, or their current metabolic status.
The discussion points to a familiar historical shift: the old food pyramid emphasized grains and starches as the base, and over the same decades, obesity and metabolic disease rose dramatically. Correlation is not causation, but the video treats this as a strong reason to re examine the default template, especially for people who are already insulin resistant.
This approach is also intentionally practical. You are not asked to memorize a list of “superfoods.” You are asked to build meals from a smaller set of satiating, nutrient dense foods, then treat carbohydrates as a variable knob you turn up or down.
The video’s core claim, 93% of adults need a different pyramid
The central claim is blunt: a “real food pyramid” for most adults should prioritize metabolic repair.
That means the food foundation is not bread, cereal, pasta, or other refined starches. The foundation is protein and minimally processed fats.
The speaker anchors this in a paper he references, “Myths and Facts Regarding Low Carbohydrate Diets,” and he notes that low carbohydrate diets have been studied for decades with thousands of clinical trials. He also emphasizes that major diabetes organizations now accept low carbohydrate patterns as an option for managing type 2 diabetes.
That point aligns with major professional guidance that recognizes low carbohydrate eating patterns as one possible approach for some adults with type 2 diabetes, depending on preferences, goals, and medication safety. For example, the American Diabetes Association’s nutrition guidance has discussed low carbohydrate patterns as a potential tool for glycemic management (ADA nutrition consensus overviewTrusted Source).
What “low carb” means here
Definitions matter because “low carb” can mean very different things.
In the video:
He also adds a practical filter: most people are not active enough to justify routinely eating far above that range.
This is not a claim that athletes should never eat carbs. It is a claim that for the average adult with a sedentary job, high carb intake can be metabolically expensive.
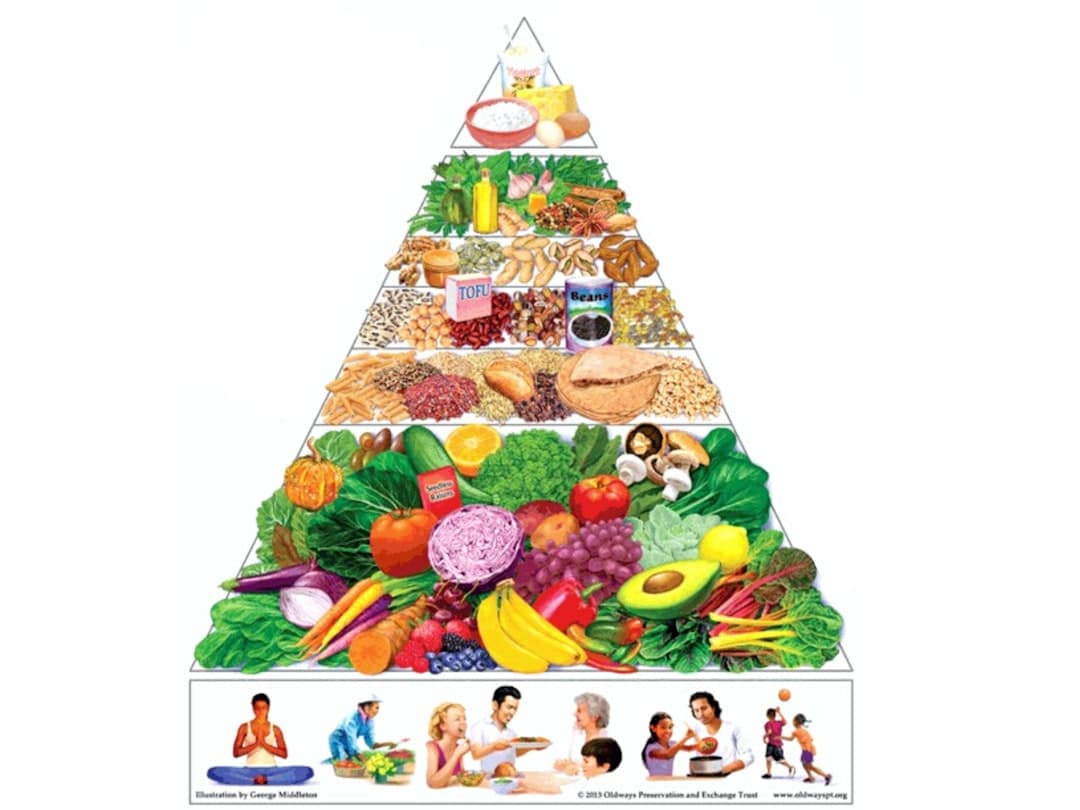
What the “real food pyramid” looks like in practice
The pyramid shown in the video flips the old model.
Instead of building your day on grains and starches, the base is made of foods that the speaker describes as more filling and less likely to be overeaten.
Here is the food foundation emphasized.
A key nuance: the video also states that if someone prefers not to eat animal fats, a low carbohydrate pattern can be built with more plant based fats.
That is important because it frames the approach as carbohydrate reduction and food quality improvement, not as mandatory carnivore eating.
Important: If you take glucose lowering medications (especially insulin or sulfonylureas), carbohydrate reduction can change your medication needs quickly. A safer move is to involve your prescribing clinician before making major diet shifts, since hypoglycemia risk can increase.
A simple “day of eating” based on the video
The speaker gives concrete examples that keep showing up in his coaching style.
This is a very different feel from the classic “toast, cereal, low fat yogurt” pattern many people were taught.
Carbs are not “bad”, they are dose dependent
The most actionable idea in the video is that carbohydrates should match what you do with your body.
If you are doing CrossFit, running, cycling, or lifting weights several days per week, the speaker argues you can “afford” more starch and fruit. If you are mostly sedentary, he suggests keeping total carbs much lower, with a number he repeats as a common target, often under 100 grams per day for many people.
This is essentially carb periodization for regular life.
It also helps explain why two people can eat the same “healthy” carb heavy diet and get different outcomes. Someone training hard may dispose of glucose into muscle more effectively. Someone with insulin resistance may see higher blood sugar and insulin responses to the same meal.
“Does the brain need carbs?”
This is where the video takes a strong stance.
The argument presented is that the brain’s dietary carbohydrate requirement is essentially zero because the body can generate glucose through gluconeogenesis (making glucose from amino acids, lactate, glycerol). The transcript states there are no deficiency symptoms even with complete absence of dietary carbohydrates, and that the small amount of glucose needed for certain tissues can be produced internally.
From a physiology standpoint, it is true that the body can maintain blood glucose without dietary carbohydrates via gluconeogenesis and glycogen breakdown. However, whether “zero carb” is the best or easiest approach for a given person depends on goals, preferences, medical history, and medication use.
If you are considering very low carbohydrate intake, it can be helpful to discuss it with a clinician, especially if you are pregnant, have kidney disease, have a history of eating disorders, or take medications that affect blood sugar.
Pro Tip: If you lower carbs quickly and feel headachy, weak, or crampy, it may be an electrolyte and fluid issue, not a sign that “your body needs sugar.” The video specifically notes that “keto flu” is often avoidable with electrolytes and hydration.
Common worries, saturated fat, LDL cholesterol, and red meat
A big part of the video is reassurance.
It addresses the fear that eating eggs, full fat dairy, and red meat automatically leads to heart disease or cancer.
Some of these topics are still debated in nutrition science, and individual risk varies. Still, the video’s unique perspective is that the common warnings are often overstated, especially when carbohydrate intake is lower and metabolic markers improve.
Saturated fat, in context
The transcript cites a 2020 review in the Journal of the American College of Cardiology arguing there were no clear benefits of reducing saturated fat for cardiovascular disease risk and total mortality.
That paper is widely discussed and provides a detailed critique of saturated fat policy and the importance of food matrices and replacement nutrients (JACC reviewTrusted Source).
The video’s framing is not “eat unlimited saturated fat.” It is closer to: if you lower ultra processed carbohydrates and improve insulin resistance, saturated fat may not behave the way people fear, and focusing only on saturated fat can distract from more meaningful metabolic drivers.
LDL cholesterol, and the “lean outlier” idea
The discussion acknowledges that LDL cholesterol can rise on low carbohydrate diets.
The key claim is that this rise is more common in lean individuals (the “lean mass hyperresponder” pattern), and that in a cited analysis, those lean outliers with high LDL did not show significantly more plaque over about 4.7 years compared with matched controls.
This is an evolving area. LDL is still considered a causal risk factor in atherosclerosis in mainstream cardiology, and many clinicians will take high LDL seriously. At the same time, the video emphasizes that other markers often improve with carbohydrate restriction, including triglycerides, HDL, blood pressure, and inflammatory signals.
A practical takeaway is that if LDL rises substantially, you do not have to guess. You can talk with a clinician about a fuller risk assessment, which may include family history, ApoB, lipoprotein(a), blood pressure, glycemic control, and sometimes imaging such as coronary artery calcium scoring.
What the research shows: Coronary artery calcium (CAC) scoring is one tool clinicians use to refine cardiovascular risk in some adults, and large guidelines discuss CAC as a risk stratifier when decisions are uncertain (ACC/AHA cholesterol guidelineTrusted Source).
Red meat and cancer, what the video argues
The transcript claims that the strongest reviews using GRADE methodology found low to very low certainty evidence linking red meat to major outcomes like heart disease, type 2 diabetes, and cancer.
This refers to a set of controversial systematic reviews published in Annals of Internal Medicine that concluded the certainty of evidence was low and that absolute risk reductions from reducing meat intake were small (Annals of Internal Medicine guideline and reviewsTrusted Source).
You do not have to interpret this as “red meat is a free for all.” A more careful translation is: the evidence is complex, much of it is observational, and individual choices can consider overall dietary pattern, cooking methods (avoiding charring), fiber intake, and personal risk factors.
Why insulin resistance is treated as the main villain
The most distinctive claim in the video is that insulin resistance is not just “one problem among many.”
It is framed as the upstream driver that initiates or accelerates atherosclerotic plaque in coronary, carotid, and cerebral arteries.
That is a strong statement, but it points to a real clinical idea: insulin resistance often clusters with high triglycerides, low HDL, high blood pressure, fatty liver, and chronic inflammation, all of which can worsen cardiovascular risk.
So the pyramid is built around improving insulin sensitivity, not merely reducing calories.
Low carb for type 2 diabetes, the remission emphasis
The transcript highlights that many clinicians think type 2 diabetes is irreversible, but remission is possible, and carbohydrate reduction has strong evidence for glycemic control.
It references a trial of people with type 2 diabetes in which more than half achieved reversal or remission on a ketogenic approach and many reduced medications quickly.
One well known example in this space is the Virta Health continuous care intervention, which reported substantial improvements in glycemic control and medication reduction over time in adults with type 2 diabetes following nutritional ketosis with remote support (Virta 2 year outcomesTrusted Source).
Remission does not mean “cured forever.” It usually means blood sugar is in a non diabetic range without glucose lowering medications for a period of time, and ongoing lifestyle support is often needed.
The practical point remains: for many people, lowering carbohydrate intake can be a powerful lever for lowering glucose and insulin demand.
Medication vs diet, and the GLP-1 note
The video also contrasts dietary approaches with medication only approaches.
It argues that some diabetes medications can lead to weight gain and do not produce remission for most people. It also mentions GLP 1 receptor agonists, saying they may help but can have side effects and high discontinuation rates.
In real world care, GLP 1 medications can be beneficial for some people, but side effects such as nausea and vomiting are common, and rare but serious risks exist. If you are using or considering GLP 1 therapy, it is reasonable to ask your clinician about side effects, what symptoms should prompt urgent care, and how nutrition changes might interact with medication.
Q: If I go low carb, should I stop my diabetes meds?
A: Do not stop medications on your own. Carbohydrate reduction can lower blood sugar quickly, which may require medication adjustments, but that should be done with the prescribing clinician to reduce hypoglycemia risk. If you use insulin or sulfonylureas, this is especially important.
Health education note, not individualized medical advice
How to apply this pyramid without making it extreme
A common failure mode is going “all in” for five days, then quitting.
This pyramid works better as a set of defaults you can repeat.
Below is a step by step way to implement the video’s approach while keeping it flexible.
Step-by-step, build your plate from the bottom up
Start with protein at every meal. Choose eggs, fish, poultry, beef, or a high protein dairy option like Greek yogurt. Protein tends to increase satiety and can make it easier to reduce ultra processed snacks.
Add minimally processed fats for satisfaction. Use olive oil, avocado, butter, or full fat dairy as preferred. The goal is not to drink oils, it is to make meals satisfying enough that you are not hunting for carbs an hour later.
Choose fibrous plants as your default carbohydrate. Non starchy vegetables and some whole fruits can fit many low carb patterns. They add volume and micronutrients with fewer glucose spikes than refined grains.
Scale starch to your activity level. If you lift weights, run, or do high intensity training several days per week, you may tolerate more fruit or starch. If you are mostly sedentary, consider a lower daily carb target, as suggested in the video.
Recheck, do not assume. If you have access to labs, track triglycerides, HDL, fasting glucose, A1C, and blood pressure with your clinician. If LDL rises substantially, ask about deeper risk assessment rather than relying on one marker.
A practical grocery list aligned with the pyramid
Use this as a starting point, then tailor for allergies, preferences, and medical needs.
»MORE: If you want to test the “carb dial” idea, create two weekly templates: a lower carb week for low activity days, and a moderate carb week for training heavy weeks. Then compare hunger, energy, and lab trends with your clinician.
Handling the transition, hydration, electrolytes, and expectations
The video calls out “keto flu” and treats it as manageable.
When carbs drop, insulin levels often drop too, and the kidneys may excrete more sodium and water. Some people feel tired, lightheaded, or crampy during that adjustment.
Practical strategies many clinicians discuss include drinking enough fluids, salting food to taste (if appropriate for your blood pressure and medical history), and paying attention to potassium and magnesium rich foods. If you have heart failure, kidney disease, or take blood pressure medications, electrolyte changes can be risky, so it is worth checking in with your clinician.
One more practical note from the livestream: movement matters even if your diet is solid. The speaker even tells a truck driver to stop every 90 minutes or so to move and to do “movement snacks.” That is a small habit with outsized metabolic benefits.
Q: Is 130 grams of carbs really “low”?
A: In the video’s framing, yes, because many adults routinely eat far more than that through bread, pasta, snacks, and sugary drinks. Whether it is “low” for you depends on your activity level, goals, and how your blood sugar responds.
Health education note, not individualized medical advice
Key Takeaways
Frequently Asked Questions
- What is the “real food pyramid” in this video?
- It is a low carbohydrate oriented pyramid aimed at improving metabolic health. The base emphasizes protein rich foods (eggs, fish, red meat), whole fat dairy, and fats and oils, with carbohydrates added in higher amounts only when activity level supports it.
- How many carbs counts as low carb or keto here?
- The video defines ketogenic eating as about 20 to 50 grams of carbs per day, and low carb as under 130 grams per day. It also suggests many adults may do well under about 100 grams per day if they are not very active.
- Does the brain require dietary carbohydrates?
- The video argues the dietary requirement is essentially zero because the body can make glucose through gluconeogenesis. If you are considering very low carb intake, it is wise to discuss it with a clinician, especially if you take glucose lowering medications.
- What if my LDL cholesterol rises on a low carb diet?
- The video notes LDL can rise in some people, especially lean individuals, while other markers often improve. If LDL rises substantially, consider discussing a fuller risk assessment with your clinician, rather than focusing on a single lab value.
- Is this approach only animal based?
- No. While the foundation emphasizes animal source proteins and whole fat dairy, the video also notes that low carb patterns can use plant based fats if someone prefers to limit animal fats.
Get Evidence-Based Health Tips
Join readers getting weekly insights on health, nutrition, and wellness. No spam, ever.
No spam. Unsubscribe anytime.